
Meniscal Repair
What is a meniscal repair?
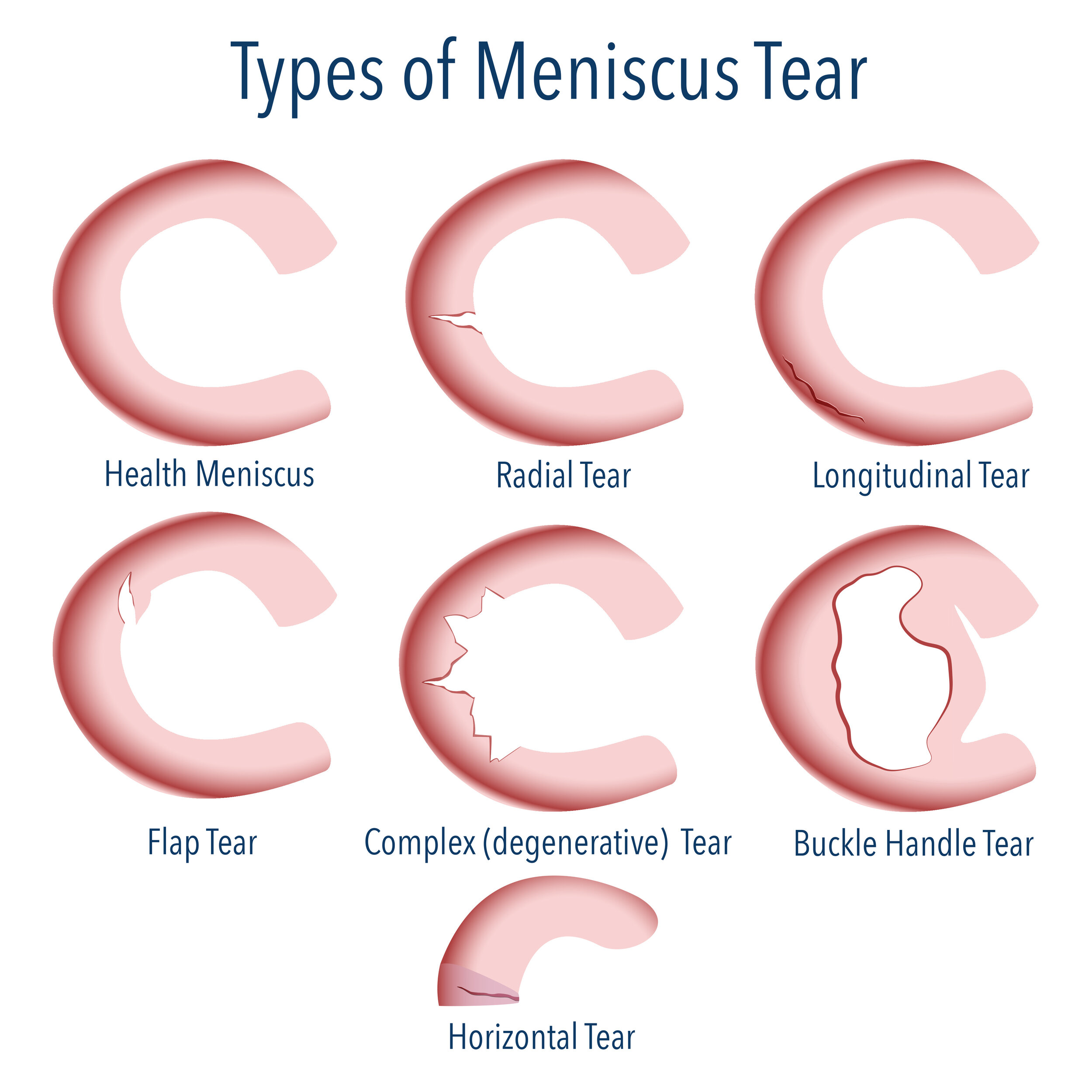
The meniscus acts like a shock absorber in the knee, protecting the cartilage. It is C-shaped, and each knee has a meniscus on the inside (medial) and on the outside (lateral). An acute traumatic knee injury can cause the meniscus to tear. A torn meniscus may cause secondary cartilage damage, knee swelling, locking, or clicking.
With age, the quality of tissue within the meniscus declines. This can cause the meniscus to tear even in the absence of any trauma. This is referred to as a degenerative tear.
A meniscal repair involves stitching the torn meniscus back into position so it is able to heal. A healed meniscal repair will restore the function of the meniscus and its ability to protect the cartilage in the knee.
What is involved in meniscal repair surgery?
The steps involved in meniscal repair surgery include:
Diagnostic Arthroscopy
2-3 small (< 1cm) portals are created to allow passage of a camera and surgical tools within the knee joint. The whole joint is inspected for damage.
Meniscal repair
The torn meniscus is repaired using stitches. If it all possible, a repair is preferable to a resection as the shock absorbing function of the meniscus is retained. Sometimes this can be performed completely via key-hole surgery using an “all-inside” surgical device.
If the tear is extensive, an accessory incision is made on the side of the knee, and sutures are passed from the inside of the knee to the outside through the open accessory incision. These stitches are then directly tied over the capsule to provide strong repair. This is considered the gold standard for meniscal repair.
Meniscal resection
In some situations, the torn meniscus is not suitable for repair and the torn portion is therefore trimmed to a stable margin. This can relieve the pain and mechanical symptoms associated with a tear. Trimming the meniscus will reduce its shock absorbing capacity and will put more pressure on the surrounding cartilage. This will cause the cartilage to wear out quicker than normal and lead to arthritis in the knee.
What is my follow-up schedule after the operation?

Meniscus tear repair arthroscopy before and after surgery - Melbourne.
Approximately 3-4 weeks of leave from work is required for a desk-based job. You may require a knee brace for up to 6 weeks to help protect the repair. Depending on the pattern of the tear and type of repair performed, you may also be restricted in the amount of weight you can place on the operated leg. In this situation you will be mobilising with crutches.
2 weeks
The wound dressings will be removed and the wound will be reviewed to ensure it has healed. The sutures will be removed at this stage.
8 weeks
The range of motion in the knee will be assessed. It is expected that you will be able to fully straighten the knee and bend it more than ninety degrees. If you have been prescribed a knee brace, it is usually discarded at this stage.
4 months
The knee should have a full range of motion but may have a small amount of residual swelling around it. If things have progressed as expected, this will be your final appointment. Return to sports can be commenced by 4-6 months post-operatively but will depend on the nature of the repair.
Frequently Asked Questions
What are the risks of having meniscal repair surgery? +
General complications of meniscal repair surgery can include:
Infection
Although the risk of infection is extremely small following a knee arthroscopy, it can still occur. A deep infection of the knee joint may require surgical washout of the knee and antibiotics.
Bleeding
Bleeding can occur around the arthroscopic port sites or into the knee joint itself. This is usually self-limiting but on rare occasions will require another operation to wash out the accumulated blood.
Deep vein thrombosis and pulmonary embolism
Clots can occur in the deep veins of the leg that may dislodge and occlude the arteries in the lungs. DVT presents as leg pain and swelling after your operation. The diagnosis is confirmed with an ultrasound scan and, depending on the type of DVT, may require treatment with blood thinners.
Specific complications of meniscal repair surgery can include:
Meniscal repair failure
If there is no healing around the site of the meniscal repair over time, the sutures used for the repair will fail. If this occurs, the meniscus will tear again and potentially become symptomatic. This may necessitate another knee arthroscopy and possible re-repair or resection of the re-torn meniscus.
Irritation from the suture anchors
Sometimes the anchors from an all-inside meniscal repair device can come loose and dislodge themselves within the knee. This can cause pain and mechanical symptoms within the knee. If this occurs, a repeat arthroscopy may be required to remove the loose anchors.
Damage to the saphenous nerve
The saphenous nerve supplies the skin over the inside of the leg. This nerve can be damaged when making an open incision to repair the medial meniscus, or when passing inside-out sutures during medial meniscal repair. This will result in numbness inside the leg. In some cases, the damage to the nerve may be permanent.
Damage to the common peroneal nerve
This is a rare risk when performing an inside-out repair of the lateral meniscus of the knee. The needle used for the repair can damage the common peroneal nerve, which supplies the muscles that pull the ankle up. Damage to this nerve causes a foot drop. If this is noted after surgery, you will require removal of the meniscal repair suture and exploration of the common peroneal nerve. In some cases, the damage to the nerve may be permanent.
Damage to the popliteal artery
This is a rare risk when repairing a lateral meniscus. The popliteal artery Is the major artery supplying the lower limb and passes behind the knee joint. When meniscal needles are being used for the repair, they may rarely puncture the popliteal artery and cause it to bleed or form an aneurysm. This may require surgical exploration and repair by a vascular surgeon.
Can the meniscus heal on its own? +
For smaller stable tears that are close the periphery of the knee joint where the bloody supply is rich, it is possible that the torn meniscus can heal. This can take 8-12 weeks to happen and is unlikely to occur in larger and more unstable tears.
Is it possible for me to make the torn meniscus worse without surgery? +
A torn meniscus can be made worse, especially in the setting of a concurrent torn ACL. In this situation, the instability in the knee can exert more pressure on the tear and propagate it. This can potentially make a repairable tear irreparable.
What’s the success rate of meniscal repair? +
The success rate of a meniscal repair is between 80-85%. The meniscal repair is designed to reappose the two torn ends of the meniscus but it still relies on the body to heal the tear. There are several factors that contribute to the success of the repair.
The blood supply to the meniscus is variable and as a result, the location of the tear will determine the likelihood of successful healing. The central part of the meniscus has a poor bloody supply so tears in this area have a low chance of healing. This contrasts with tears in the periphery of the meniscus which have a rich bloody supply and a high chance of healing.
If the meniscal tissue is of poor quality and the tear is degenerative in nature, this has a low likelihood of healing and a repair is unlikely to be successful.
If the meniscal repair is performed in conjunction with an ACL reconstruction, it is more likely to heal. This is thought to be because of the release of growth factors into the knee from the bone bleeding that occurs when the tunnels for the ACL reconstruction are being created.
Other factors such as the configuration of the meniscal tear and how long the tear has been present for will also contribute to the success.
If the repair fails, it will present with pain and swelling within the knee. An MRI scan will confirm failure of the meniscal repair. In this situation, a re-repair can be performed or a trimming of the torn meniscus.
Why don’t you just remove the torn meniscus? +
The normal function of the meniscus is to protect the cartilage in your knee. Trimming even 20% of the meniscus can increase the pressure on the cartilage in the knee by up to 300%. This can lead to accelerated cartilage wear and subsequent arthritis.
If the meniscus is able to be repaired, this is the best option. The disadvantages are the prolonged recovery time, need for a knee brace and limited weight bearing after the operation and the risk of failure.
If the repair fails, the torn meniscus can still be trimmed. Although most failures occur within 12-18 months of the repair they can occur later than this time frame.
In athletes, removing a significant portion of the lateral meniscus can be a career limiting injury. This inevitably causes fast wear in the lateral compartment of the knee and an early retirement from sports.
What is a meniscal cyst? +
Meniscal cysts usually occur in conjunction with meniscal tears. It is thought that the meniscal tear allows fluid within the knee joint to leak through the tear and cause the cyst to form. If the cyst is large enough, it can cause discomfort from the pressure it exerts on the surrounding soft tissues. Meniscal cysts are treated by attending to the meniscal tear and excising the cyst. Sometimes the cyst can be excised using arthroscopic (key-hole) surgery, and other times an open incision is required.