
Osteochondritis Dissecans
What is osteochondritis dissecans?
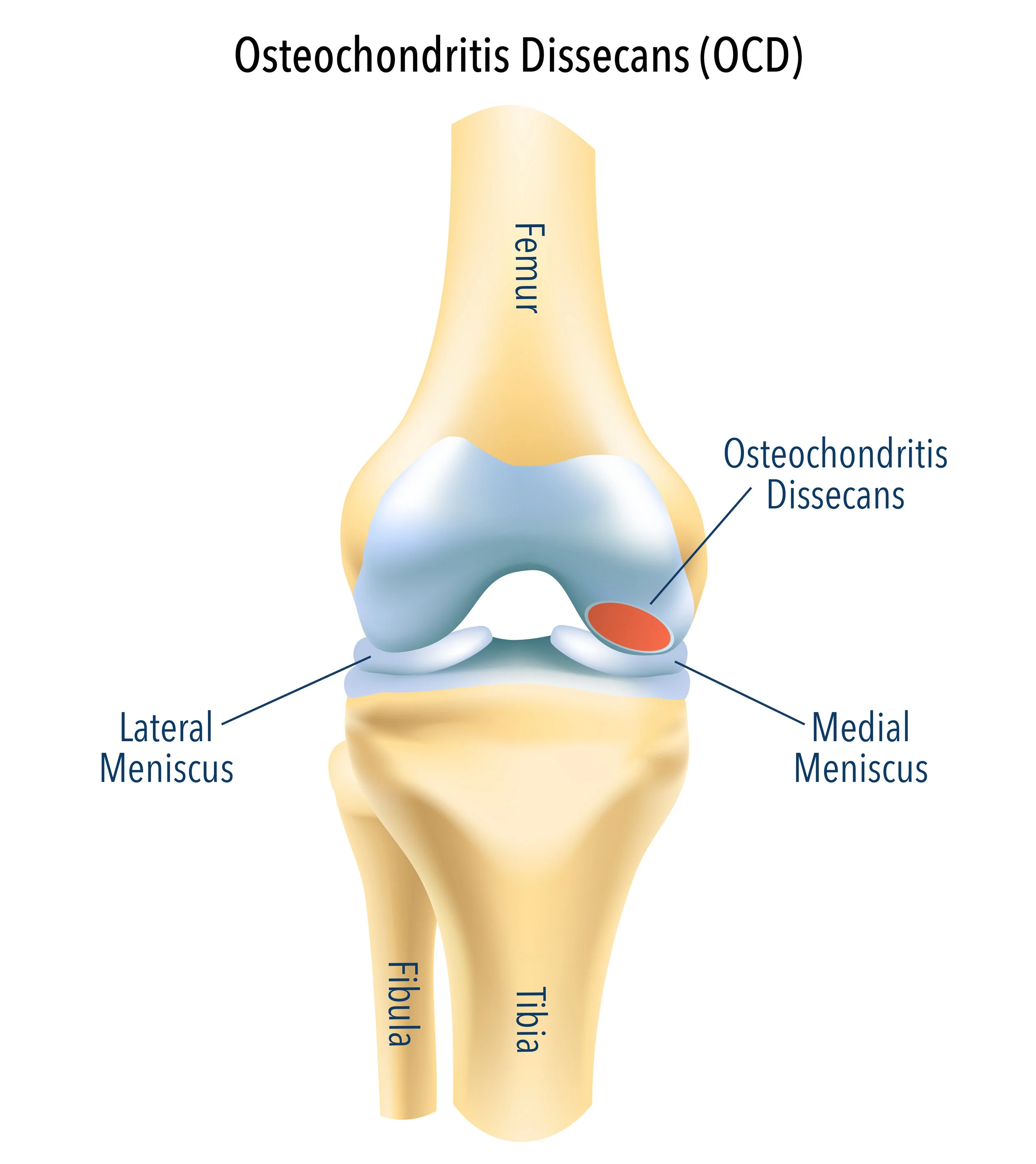
Osteochondritis dissecans is an abnormal condition involving the cartilage and underlying bone within the knee joint. Although there are many theories as to what causes this condition, the exact cause still remains unknown.
This condition usually affects children and young adults, and the lesion is usually located in the medial femoral condyle.
With time and repetitive micro-traumas, the disease part of cartilage and bone may detach from its surroundings and float within the knee joint as a loose body. If this remains untreated, the long-term sequalae is secondary arthritis of the knee joint.
What are the symptoms of osteochondritis dissecans?
This condition can present with knee pain and swelling within the knee joint. The pain typically is worse with activity. If there is a loose fragment of bone and cartilage, as is seen with advanced cases of the disease, it may cause clicking or locking of the knee joint.
How do you treat osteochondritis dissecans?
Initially, X-rays and an MRI scan will be obtained. In certain cases, a CT scan may also be obtained. This will determine the fragment size and instability.
Stable lesions can be managed with activity restriction and protected weight bearing. In these situations, a follow-up appointment with repeat imaging is necessary to ensure the lesion is healing and the knee pain and swelling is settling.
Surgery is usually indicated for unstable lesions or stable lesions that don’t respond to non-operative therapy.
What does surgery for osteochondritis dissecans involve?
The type of operation depends on the size and stability of the lesion. The best outcome is retention and healing of the osteochondral fragment. Unfortunately, this is not possible in all cases, which is why there are multiple options for managing this situation.
Removal of loose fragment
This involves removal of the unstable osteochondral fragment with arthroscopic (keyhole) surgery.
In-situ drilling of lesion
Small drill holes are made through the cartilage and underlying bone in the lesion to stimulate a healing response. This is usually performed with keyhole surgery.
Fixation with or without bone grafting
When the osteochondral lesion is unstable and is of sufficient size, it can be repaired back to the donor site using absorbable pins or metal screws. This is performed by keyhole or open surgery depending on the location of the fragment. If there is a loss of bone at the donor site of the fragment, this can be built up by using your own bone graft. The fragment is then repaired over the bone graft as a single-stage procedure. The bone graft is usually sourced from your femur or tibia bone.
Excision of lesion and marrow stimulation
The osteochondral lesion is removed and the underlying bone is drilled in order to stimulate new cartilage formation. Although the new cartilage is not microscopically like the joint cartilage you are born with, it acts as effective buffer to cover the site of the lesion. This form of treatment is effective in small to moderate sized osteochondral lesions that are not able to be repaired.
Autologous chondrocyte implantation with or without bone grafting
This is a 2-stage procedure. The first stage involves performing keyhole surgery to harvest cartilage cells from your knee. These cells are cultured and grown in a laboratory and are then placed on a collagen-based scaffold, which provides an environment that encourages growth of the cartilage cells. The second stage involves re-implanting the grown cells on the collagen scaffold back into the knee in the area of cartilage loss. This procedure is performed when repair of the cartilage lesion is not possible and the defect is moderate to large in size. It can be performed in conjunction with bone grafting.
Osteochondral allograft
Part of a knee joint from a cadaver (dead human tissue donor) is sourced and then surgically fashioned to match the area of cartilage loss in your knee. Your knee is then surgically prepared to accept the cadaveric graft, which is then press-fit into place. Occasionally metal screws are inserted through the allograft to provide additional stability. Your own bone cells grow into the allograft bone, and the graft will incorporate with time. This surgery requires an open incision and is suitable for large osteochondral defects.