
Patellofemoral Instability
What is patellofemoral instability?
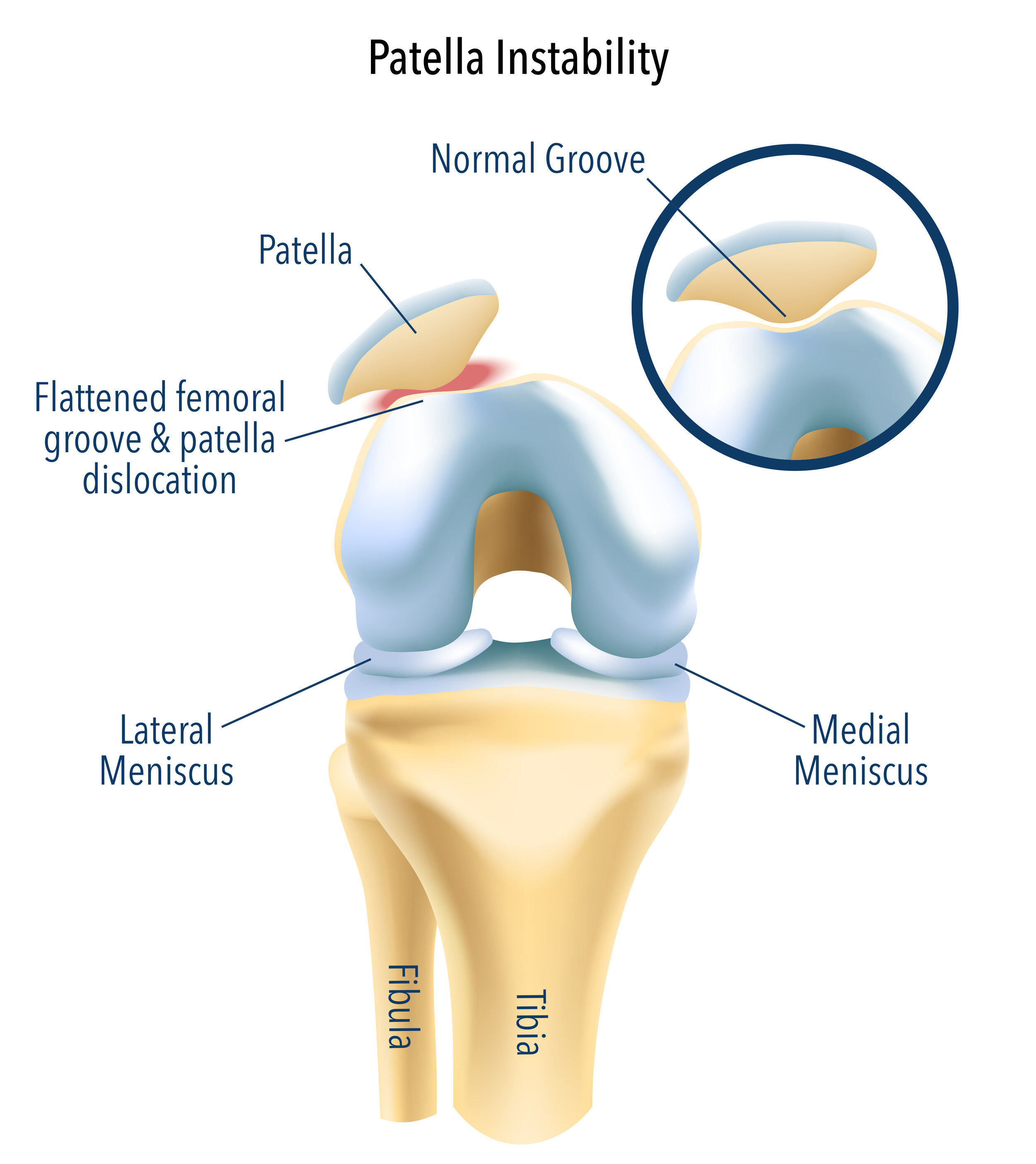
The patella (kneecap) is an important bone that improves the vector of force for the quadriceps muscle. It normally glides with knee movement within a v-shaped groove in the femur.
The patella can partially or completely slide out of this groove with a twisting knee injury, direct blow, or a fall. When this occurs, the patella usually dislocates to the outside (lateral) aspect of the knee. Sometimes the patella falls back into its normal position by itself, and other times it needs to be put back in its place by paramedics or emergency staff.
What are the symptoms of patellofemoral instability?
Patients can experience frank dislocation where the kneecap completely slides out of its normal position. This will present with pain, swelling, and a change in the appearance of the knee.
The patella may also partially slide in and out of its normal position with day-to-day activities and present with pain and apprehension as these episodes occur.
How do you treat patellofemoral instability?
The treatment for a first-time dislocation is usually non-operative. Mr Pai will arrange an MRI scan to make sure that there aren’t any loose fragments of bone or cartilage within the joint, which sometimes occurs with patella dislocation. The MRI will also help define other risk factors that may predispose you to repeated dislocations.
Assuming there are no loose fragments in the joint, Mr Pai will then refer you to a physiotherapist to build up the strength of the thigh and buttock muscles, which can act to stabilize the patella in its groove.
If there are ongoing episodes of instability despite adequate rehabilitation, then Mr Pai will discuss surgical management with you. In addition to an MRI scan, you may require plain X-rays of your knee, an X-ray from your hips to your ankles to look at the alignment of your bones, and a CT scan to look at the rotation of the bones in your lower limbs.
There are certain anatomical problems that predispose patients to having recurrent instability. These include issues with the development of the V-shaped groove in the femur (trochlear dysplasia), the height of the kneecap in relation to the tibia (patella alta), and issues with the alignment or rotation of the lower limb. It is important to address these issues and formulate an individualised operative plan.
What does surgery for patellofemoral instability involve?
If non-operative measures prove unsuccessful and patients experience recurrent dislocations or feelings of instability during activities or sport, then surgery can be considered.
The operative plan will be based on the anatomical causes of instability. Several operations can be performed in isolation or in conjunction that are described below:
Medial patellofemoral ligament reconstruction
This involves reconstructing the ligament on the inner aspect of the kneecap that acts like a tether to prevent dislocation. This ligament ruptures or gets stretched during the first episode of patella dislocation. The operation involves harvesting one of the hamstring tendons and then attaching it to the kneecap and the inner aspect of the femur bone to recreate the tether.
Tibial tuberosity osteotomy
The kneecap is connected to the tibia via the patellar tendon. The patellar tendon inserts onto a bony prominence on the tibia called the tibial tuberosity. This operation is designed to correct the abnormality when the kneecap is in a higher position than normal or the alignment of the kneecap is not right.
The osteotomy involves detaching the tibial tuberosity and reattaching it to the tibia in a different position, which is biomechanically favourable and allows for stable patella tracking. The tibial tuberosity is reattached using screws and a small plate. This procedure is not recommended for growing children, as the osteotomy will affect the growth plate in the tibia.
Trochleoplasty
When the V-shaped groove (trochlea) of the femur in which the patella is seated during normal knee movement is not properly formed, this will predispose the patient to patella instability. This condition is termed trochlear dysplasia.
A trochleoplasty is an operation designed to recreate the groove by lifting the cartilage and reshaping the bone underneath the cartilage to form a valley. The cartilage is then reattached to the bone and allowed to heal.
There are different grades of trochlear dysplasia, and a trochleoplasty is not recommended in most cases of mild to moderate dysplasia, as it is a complex operation with a prolonged recovery. This procedure is also not recommended for growing children, as the trochleoplasty can affect the growth plate in the femur.
Derotational osteotomy
When the femur and/or tibia are malrotated, this can create an abnormal force vector that predisposes the patella to dislocation. This malrotation can be screened for during clinical examination and be quantified by performing a special type of CT scan.
If this malrotation is significant, it may need to be corrected by making a cut through the involved bone (femur and/or tibia) and rotating it to a normal position. The bone is then held in this position either using a plate and screws, or a rod through the centre of the bone with screws.
Mr Pai will perform a full clinical and diagnostic investigation to determine which operations are suitable in your case.